Bullous Myringitis
A 4-year-old male is brought to the Pediatric emergency department (ED) at 1 am for a complaint of severe ear pain. He was in such discomfort that his mother was concerned he had poked himself in the ear before bedtime while “aggressively” cleaning his ears with a Q-tip. However, she denies seeing any blood and he has been otherwise well without fever or congestion. A physical exam revealed an uncomfortable child holding his hand over his right ear.
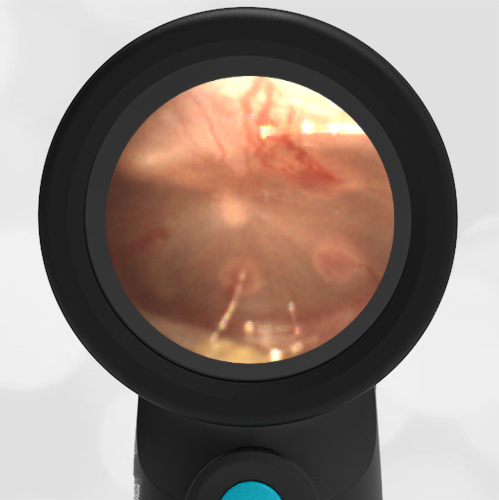
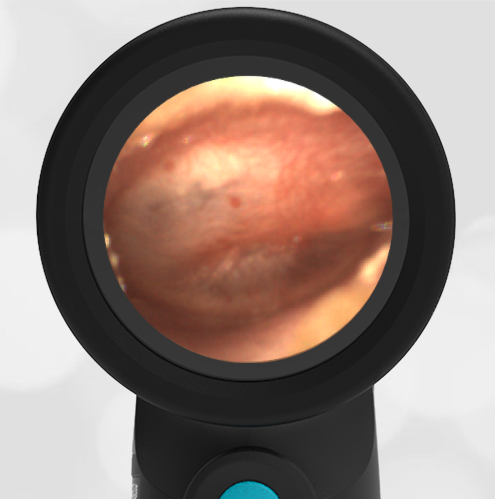
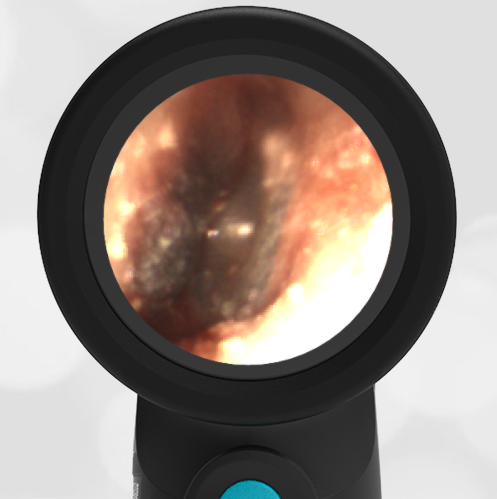
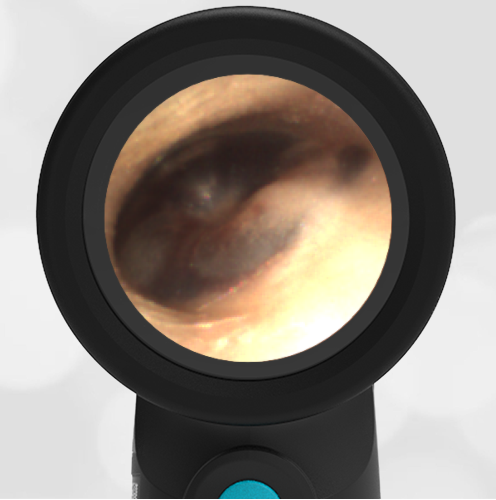
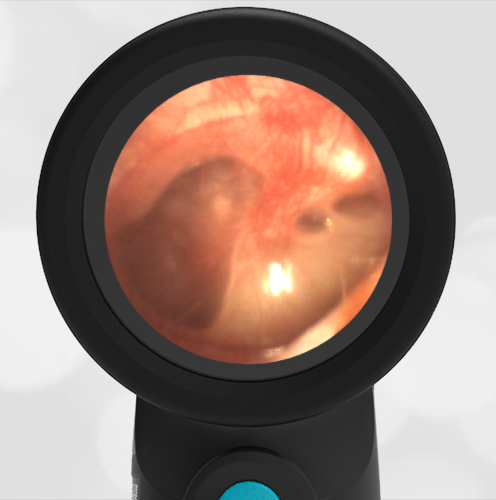
The Wispr exam is shown below.
What is your diagnosis, and how could the pain be managed quickly?
The child has bullous myringitis. Topical analgesics will help reduce the pain.
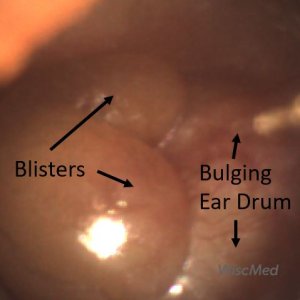
It is understandable why this child is so miserable as he has severe bullous myringitis. This is often considered to be on the spectrum of acute otitis media. The two large blisters and tympanic membrane bulging make identification of any middle ear landmarks impossible. The severity of this case is unusual, but the initial management is not. Alcaine (proparacaine) drops were instilled into the ear and a dose of oxycodone was provided in the ED. Within 20 minutes the child reported significant relief and was discharged home on scheduled ibuprofen and a course of antibiotics (see this case for a discussion of usual pathogens). Due to the severe degree of his case, it was also recommended he follow up closely for resolution of the inflammation and audiology if any hearing concerns.
Several studies have previously demonstrated the beneficial effect of topical anesthetic in treating the pain associated with otitis media, most recently a 2008 study in the Journal of Family Practice investigated the use of 2% lidocaine (which is readily available in EDs as the IV formulation) as a topical anesthetic instilled into the ear canals of children presenting with AOM. J Fam Pract. 2008 Jun; 57(6): 370–373.
Here is the complete video exam:
Complete exam video