Resolving AOM – April 13, 2023
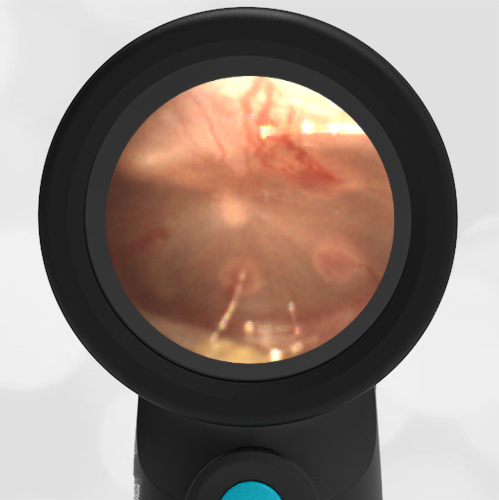
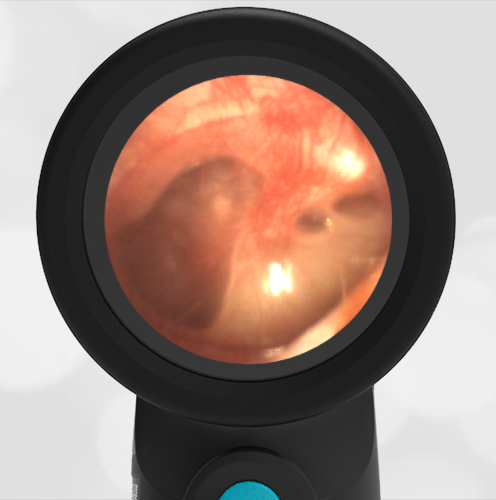
A 20-month-old presented to the emergency department (ED) due to concern about an ear infection. Mom reports her daughter has “chronic” nasal congestion and was treated a month ago for acute otitis media (“again!”). The child has not reported any ear pain, but her mom noted her “sticking her finger in her ear today.” She has had no recent fevers. She is otherwise well appearing with an unremarkable exam. Her Wispr digital otoscope exam is shown.
Which of the following is true regarding the child’s ear findings?
- The child has a profoundly bulging tympanic membrane (TM). Antibiotics are indicated to treat her acute otitis media (AOM).
- Sclerosis is present.
- The white patch at the 8 o’clock position is a result of a resolving ear infection.
- The child has an erythematous (red) TM. An urgent consult with ENT is indicated.
The answer is 3. The white patch at the 8 o’clock position is a result of a resolving ear infection.

The child’s tympanic membrane (TM) is mildly bulging as evidenced by the loss of boney landmarks and the presence of a depression/dimple in the central TM where the fixed attachment of the umbo is located. The TM does not have the classic “donut” appearance that is characteristic of moderate to severe bulging, thus acute otitis media (AOM) cannot confidently be diagnosed. There is some purulent appearing material that is adherent to the inner TM surface. At the 8 o’clock and 10 o’clock positions, this material has coalesced into patches. These patches are common findings in children with frequent AOM and are typically found one to eight weeks post-infection. They are thought to be from residual debris associated with the AOM inflammation cascade. Their presence is a hint of a resolving ear infection. Sclerosis is often present after ear infections or ear tube placement. However, in this case, there is no evidence of sclerosis. If you look closely, erythema near the periphery of the patches can be distinguished as blood vessels. These “sentinel vessels” likely are also responses to the inflammation in the middle ear and are another characteristic finding of resolving AOM.
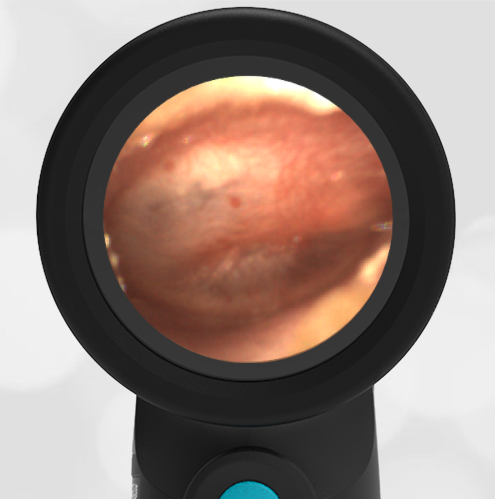
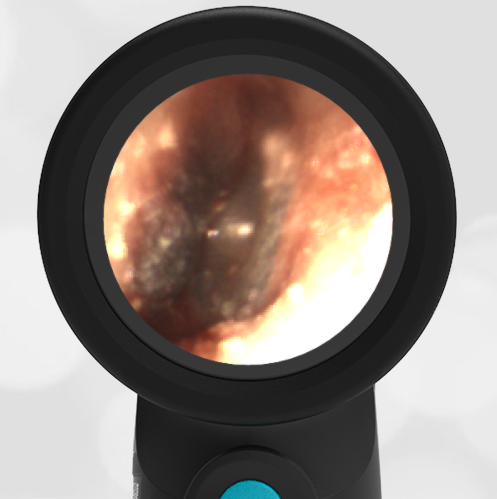
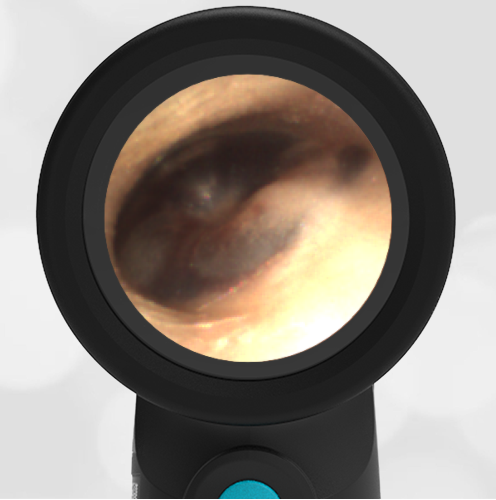
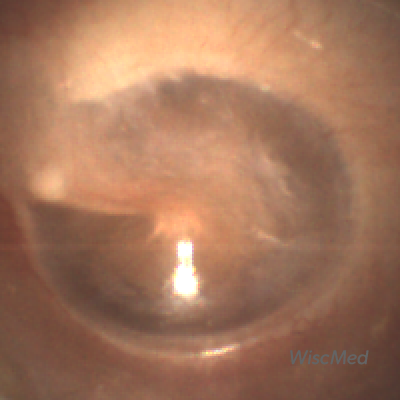
Compare the following; a normal ear, this week’s case, and a severe case of acute otitis media.
-
- Normal
-

- Resolving AOM
-

- AOM
The mother should be given return instructions in the event of ear pain or fever.
WiscMed has created a visual diagnosis guide to common ear conditions. This guide can be found here.
Here is the complete video exam: