Acute Otitis Media – Feb 1, 2024
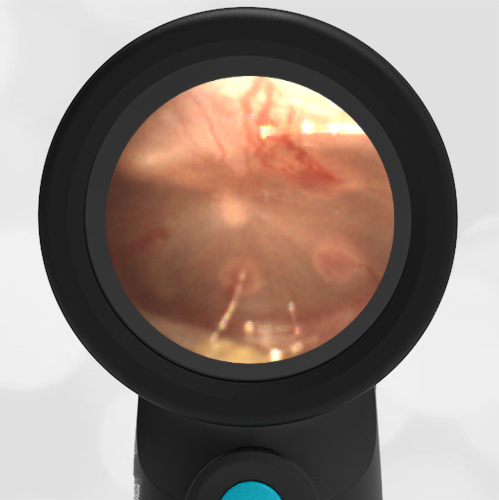
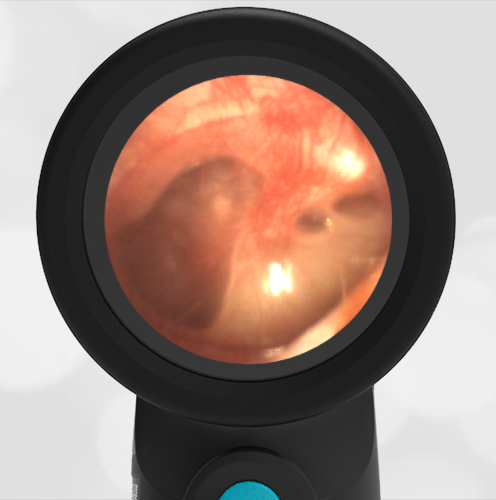
A 5-year-old female is brought into the pediatric clinic by her mother with concern for right-sided ear pain. The pain began about a day ago and has been managed well with over-the-counter analgesics. Prior to the pain developing, the child had several days of viral symptoms including cough and rhinorrhea. On exam, the child appears unwell, but not toxic. She interacts appropriately. She has a normal temperature and evidence of a runny nose. A frequent cough is noted. The child does not have a history of ear infections. The Wispr digital otoscope exam of her right ear is shown.
What is the next step in management?
- The child has mild acute otitis media (AOM) and a delayed prescription for antibiotics should be considered.
- The child has a middle ear effusion, and no further care is required.
- The child has bullous myringitis and antibiotics should be started.
- The child should be referred to otolaryngology (ENT) for ear tube placement.
Answer 1. The child has mild acute otitis media and a delayed prescription for antibiotics should be considered.
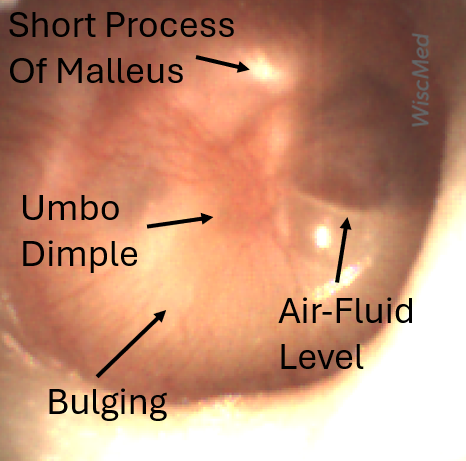
The air-fluid levels present in this image could suggest a middle ear effusion. However, the presence of bulging along with the loss of bony landmarks makes it clear that pressure is building in the middle ear space. Note that only the short process of the normally prominent malleus is visible. When acute otitis media is first developing, it is common to have air-fluid levels as the accumulation of inflammatory fluid in the middle ear starts to displace the air normally found there. Bullous myringitis is a severe form of AOM whose hallmark is blistering of the tympanic membrane.
Based on American Academy of Pediatrics (AAP) guidelines, this presentation of AOM (mild bulging, no fever, pain well-controlled) would be considered either mild or moderate. Compare this case with a case of severe bulging. In a 5-year-old with non-severe AOM, the AAP guidelines are 48-72 hours of observation with a delayed antibiotic prescription. These guidelines can be found here.
Because the child has no history of AOM and the mildness of this presentation, there is no indication for referral to otolaryngology for ear tubes.
WiscMed has created a visual diagnosis guide to the most common ear presentations that can be found here.