Myringosclerosis and Myringoplasty – April 4, 2024
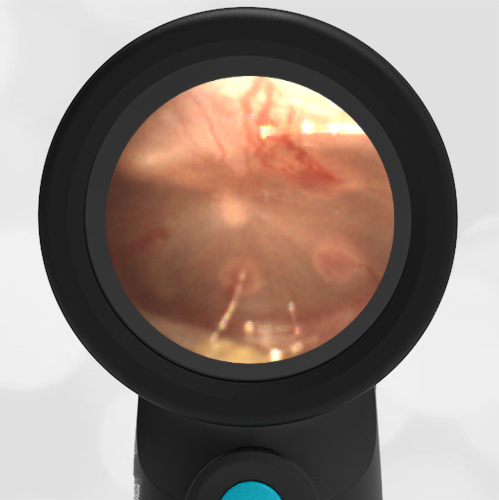
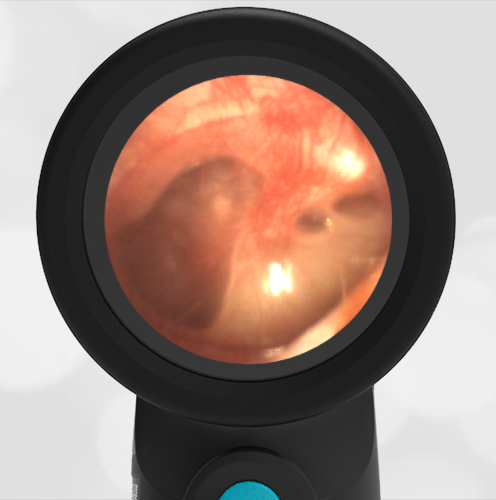
A 6-year-old presented to an Urgent Care (UC) with fever for 5 days. His mother reports he has had an upper respiratory infection for the past week and recently tested negative for influenza. This morning he felt warm, complained of headache, and had an increased nasal discharge. His parents called the nurse triage line and were directed to the UC where his temperature was 103.7oF. His Wispr digital exam is shown below. Aside from copious nasal discharge, the remainder of his physical exam was unremarkable.
Which of the following is true regarding this child’s presentation?
- He has acute otitis media (AOM) and antibiotics should be considered.
- He has a history of ear infections.
- He likely suffers from conductive hearing loss.
- He has a middle ear effusion.
Answer: B. He has a history of ear infections.
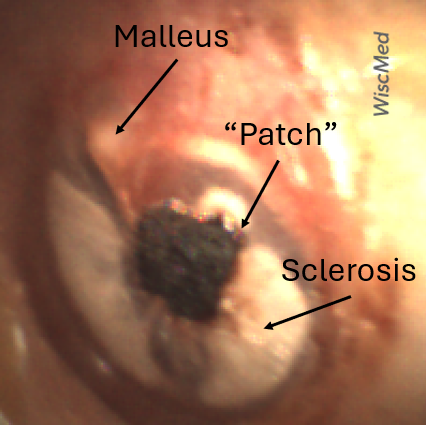
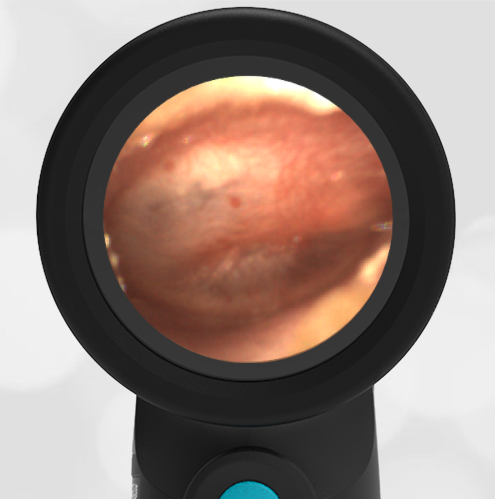
While the child’s clinical scenario of persistent fever, headache, and green nasal discharge is suggestive of sinusitis requiring antibiotics, his ear findings do not support the diagnosis of acute otitis media (AOM). However, the child’s Wispr exam does demonstrate impressive myringosclerosis characterized by the white plaques along the periphery of both tympanic membranes (TM). Myringosclerosis is a condition of calcification and hyalinization of the TM that may occur in the setting of chronic inflammation from recurrent ear infections, trauma, or following tympanostomy tube (TT) placement. Despite its appearance, myringosclerosis does not typically result in hearing loss. There is no fluid behind the TM which would be the hallmark of a middle ear effusion.
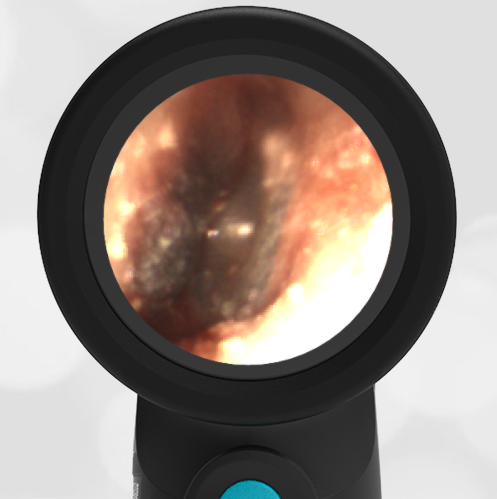
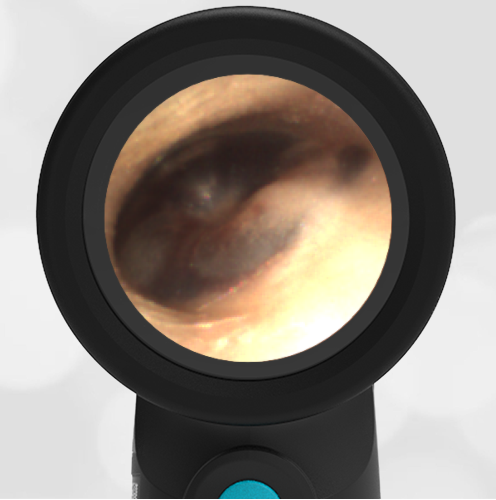
The child also has dark clotted-appearing areas, “patches,” that are not consistent with myringosclerosis. Further questioning of the parents elicited a past medical history that included frequent ear infections as a younger child. He had TTs placed four years ago which were noted to still be present at his most recent health maintenance visit. TTs typically fall out within 18 months and may cause chronic perforation if they have not spontaneously extruded by three years. For this reason, the child had the tubes removed one month prior. The darkened areas are the Gelfoam myringoplasties that were also performed to patch the resulting defects and promote healing.
Here is the complete video exam.