Seborrheic Dermatitis
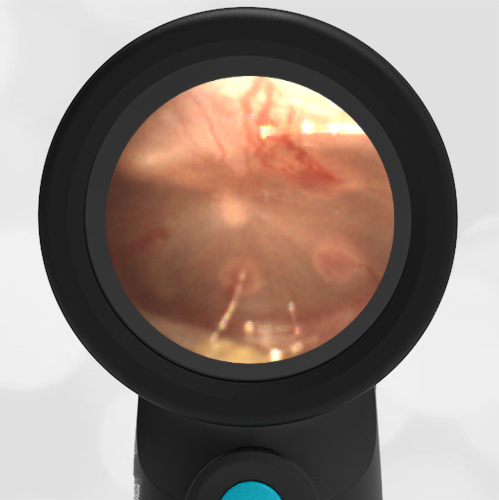
A 3-year-old male presents to the emergency department (ED) for evaluation of ear pain. Mom reports that he collided with an adult while on a trampoline two weeks ago when he was struck particularly hard by his “large” uncle’s knee in the temporal region. The child initially had a headache which has resolved. However, since the injury, he continues to complain intermittently of right ear pain that is worsened by lying down. He has not had fevers or other signs of illness. When mom spoke to his primary doctor’s office, they directed him to the ED for evaluation due to the concern for a head injury. In the ED, the child is very well-appearing without external signs of injury—no hematoma or ecchymosis. Wispr exam did not demonstrate hemotympanum but did reveal the likely cause of his ear complaint.
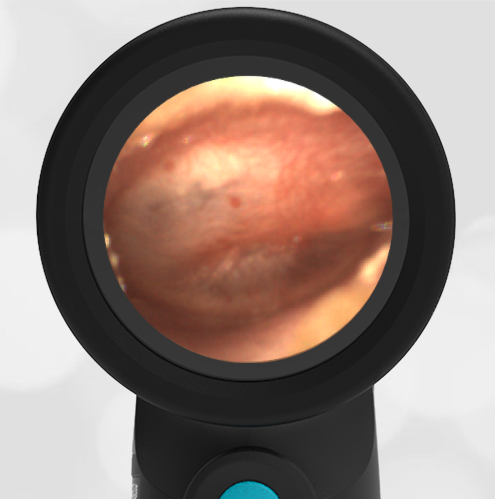
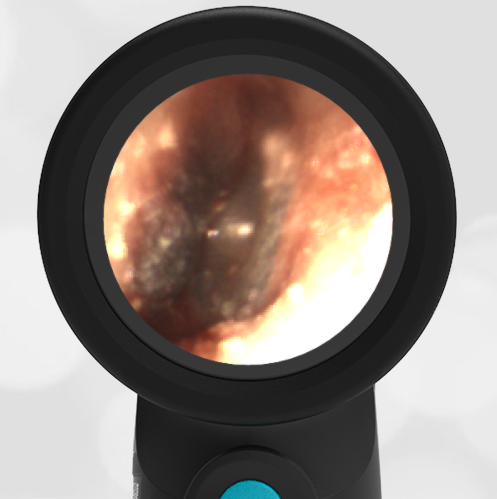
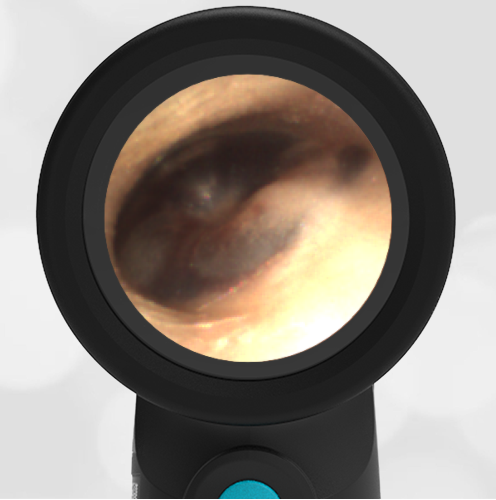
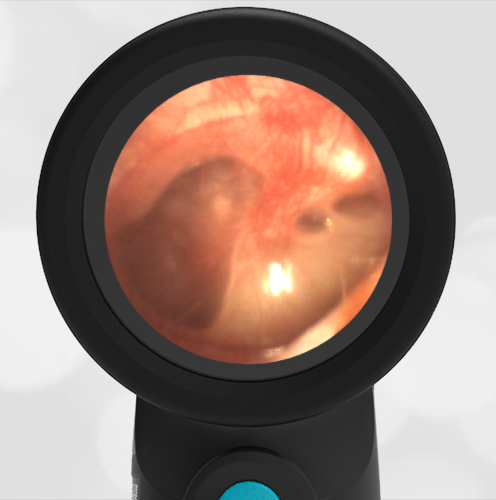
The child has seborrheic dermatitis of the external auditory canal.
While this child was sent to the ED given his reported head injury and ear pain, thankfully this was a historical red herring as the patient showed no signs or symptoms to suggest significant injury. On the contrary, Wispr exam shows that he has scaly, dry skin extending deep into the external auditory canals. In particular, his right external auditory canal (EAC) was filled with white-yellow exudative material. When commenting to the mom about the scaly findings, she noted that “he always has flaking in his scalp” as well. The last bit of additional information helped confirm the diagnosis of seborrheic dermatitis.
Seborrheic dermatitis is well-known by most clinicians to occur in the neonatal period, but this condition of inflamed, itchy skin can occur at any age. Commonly affected sites include the scalp, eyebrows, and posterior auricular areas but may include the ear canal as observed in our patient. While the differential diagnosis includes bacterial otitis externa (swimmer’s ear) or other forms of dermatitis (atopic or contact), the lack of pain with manipulation of the canal, no prior history of prolonged water immersion, and the presence of flaky scalp all support the diagnosis of seborrhea. It is interesting to note that the tympanic membrane (TM) of the right canal has patchy opacities but no bulging and normal malleus is visible. Presumably, the patchiness of the external surface of the TM is a consequence of having inflammation in the EAC and the lack of bulging or middle ear effusion (MEE) suggests there is no middle ear involvement. Treatment for this patient was steroid ear drops followed by clotrimazole ointment. This can be applied gently with a Q-tip and has the added benefit of a greasy barrier that will help calm the inflamed skin.
Here is the video exam of the right ear:
Complete exam video