Myringoplasty
A three-year-old child presents to the emergency department (ED) with vomiting and diarrhea. She had recently been seen in the pediatric clinic following a procedure to remove her ear tubes. The child is afebrile with normal age-appropriate vital signs. She is well-appearing.
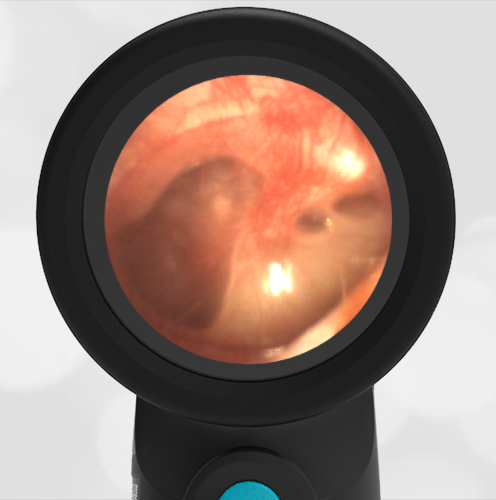
What abnormality is present in her Wispr otoscope ear exam?
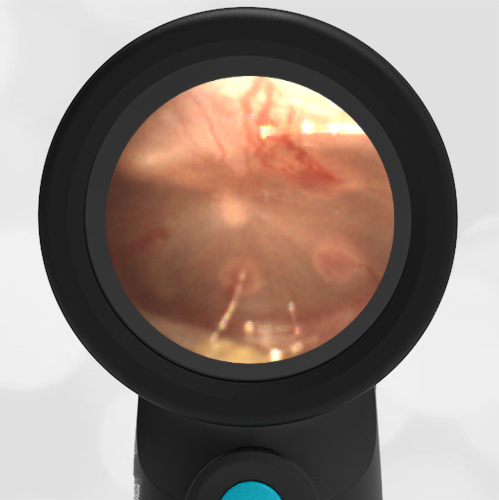
There is a patch (myringoplasty, MP) to the anterior inferior tympanic membrane (TM, ear drum).
Additional medical history for our patient included recurrent acute otitis media (AOM) throughout her first year of life resulting in tympanostomy tube (ear tube, ventilation tube) placement. The child had done very well with fewer episodes of otitis media, however, at her three-year well-child visit it was noted her left tube was still in place. Therefore, she underwent removal and paper patch myringoplasty (MP, see arrow below). Today’s exam shows the well-positioned patch. In addition, the malleus bone is discernable, and the tympanic membrane (TM, ear drum) is normal suggesting a properly healing repair without evidence of infection.

Tubes are placed in the anterior inferior quadrant of the ear drum. They typically fall out on their own in 6 to 18 months with removal being recommended if the tubes are present after two to three years. For spontaneously extruded tubes, persistent TM perforation occurs in 2% of patients with short-term tubes and 16% with long-term tubes. However, in children requiring surgical tube removal, persistent TM perforation is generally anticipated and myringoplasty via insertion of paper (such as in our patient), steri-strips, gel foam, or a collagen matrix patch is performed to encourage closure. While the reported success rates for myringoplasty techniques vary, a recent meta-analysis suggests no difference in perforation closure between patching versus no patching, regardless of the material used by the surgeon. In another study, 13% of children undergoing this procedure still had persistent perforation. Factors influencing persistent perforation included patient age, number of tubes previously placed, perforation size, and presence of myringosclerosis.
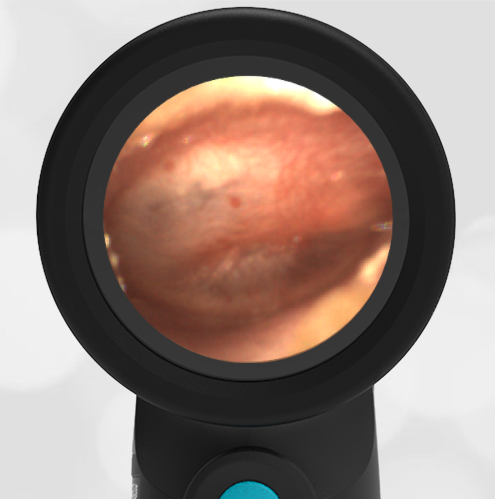
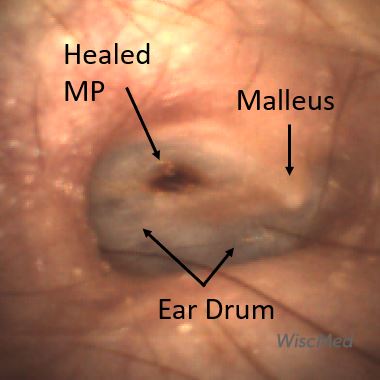
Here is an example of a healed myringoplasty.

The patient’s presenting symptoms of vomiting and diarrhea were felt to be secondary to gastroenteritis, unrelated to her myringoplasty. After an oral dose of anti-nausea medication and a successful oral fluid challenge, she was discharged home with supportive measures. No further action about her myringoplasty was necessary at today’s encounter.
Here is the complete video from the exam.
Complete exam video
Michel M, Nahas G, Preciado D. Retained Tympanostomy Tubes: Who, What, When, Why, and How to Treat. Ear Nose Throat J. 2020 Aug 31.
Tan GX, Hamilton A, MacArthur C. A Systemic Review and Meta-Analysis: Timing of Elective Removal of Tympanostomy Tubes. Laryngoscope. 2022;132(10).
Brown C, Behar P. Factors affecting persistent tympanic membrane perforation after tympanostomy tube removal in children. Int J Pediatr Otorhinololaryngol. 2020 Mar;130.