Acute Otitis Media – October 5, 2023
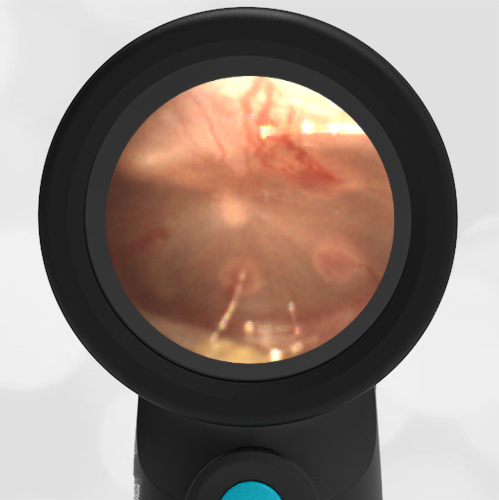
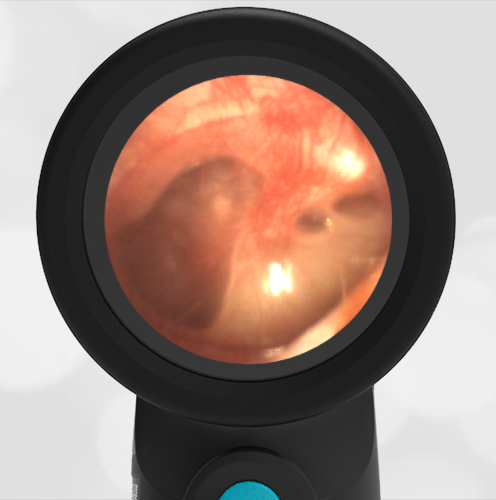
A 20-month-old male presents to the emergency department (ED) with a complaint of congestion for the past three days. Dad reports the child is in daycare and has recently been treated for croup with oral corticosteroids. The child was brought to the ED because overnight he was fussing and said that his right ear “owied.” He received a dose of ibuprofen and was able to return to sleep. In the ED his temperature is 38.5 C, respiratory rate is 32, and Pox 97%. He is overall well-appearing, smiling, and interactive without acute distress or obvious discomfort. The child has mild nasal congestion with clear rhinorrhea, but breath sounds are normal. His Wispr digital otoscope exam is shown.
Which of the following is true of the child’s diagnosis and management?
- The child’s ear is normal.
- The child has exostosis. No further management is needed.
- The child has acute otitis media and should be either (1) treated immediately with antibiotics or (2) offered close follow-up and provided with a delayed antibiotic prescription.
- The child has bullous myringitis and should be prescribed antibiotics with careful return instructions.
Answer C. The child has acute otitis media and should be either (1) treated immediately with antibiotics or (2) offered close follow-up and provided with a delayed antibiotic prescription.

The child has moderate bulging as evidenced by an inability to visualize the middle ear ossicles along with a dimple at the umbo of the malleus. These findings occur due to increased pressure in the middle-ear space from Eustachian tube dysfunction that causes pressure and fluid accumulation. Moderate bulging alone is not enough to diagnose AOM since crying, fever, and Eustachian tube dysfunction may appear similarly. According to the AAP Practice Parameter:
Clinicians should diagnose acute otitis media (AOM) in children who present with moderate to severe bulging of the tympanic membrane (TM) or new onset of otorrhea not due to acute otitis externa.
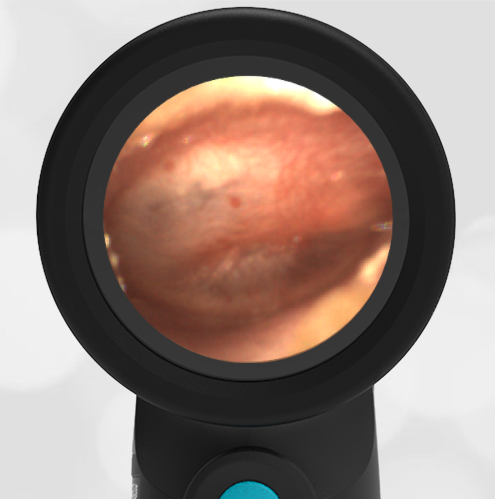
In this case, the child indicated ear pain that started overnight and was severe enough to interfere with his sleep. Since this would satisfy both the presence of pain as well as an acute onset of the symptom, the patient should be diagnosed with AOM. Of note, the patient’s left ear was normal, see image below.
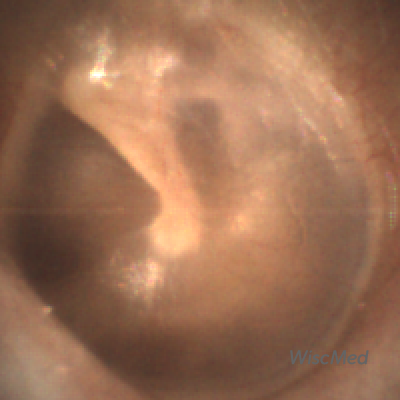
Normal Left Ear
The treatment options for AOM are dependent on several factors, including a severity assessment and age. In this case, the child appears to have relatively mild severity as his pain (while it woke him up) seems well-controlled with ibuprofen and he has not had a high fever. His left TM was normal; thus, this is a 20-month-old with non-severe, unilateral AOM. According to the AAP Practice Parameter:
Non-severe unilateral AOM in young children: The clinician should either prescribe antibiotic therapy or offer observation with close follow-up based on joint decision-making with the parent(s)/caregiver for unilateral AOM in children 6 months to 23 months of age without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39°C [102.2°F]). When observation is used, a mechanism must be in place to ensure follow-up and begin antibiotic therapy if the child worsens or fails to improve within 48 to 72 hours of onset of symptoms.
After a discussion with the child’s father, he elected to observe for worsening symptoms and arrange for follow-up if needed. A prescription was called into their pharmacy to be filled if the child developed increasing pain, persistent pain, or higher fevers.
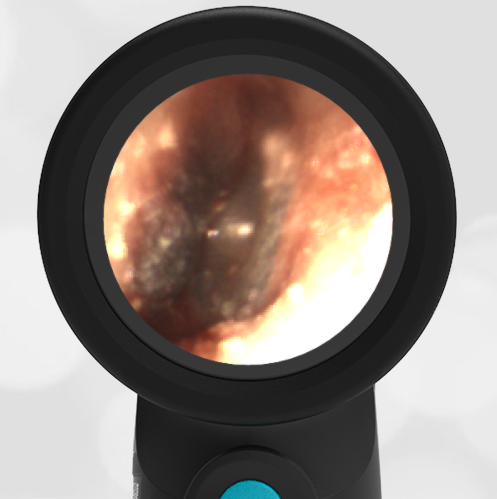
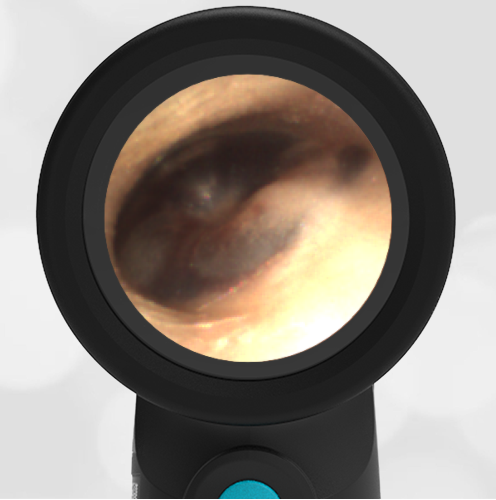
Here are examples of a normal ear, exostosis, and bullous myringitis. A normal ear is concave, the middle-ear ossicles are visible and there is a light reflex. Exostosis is a bony growth in the external ear canal that is associated with cold water activities like surfing. Bullous myringitis is a severe form of acute otitis media that presents with blisters on the ear drum.
-

- Normal Ear
-
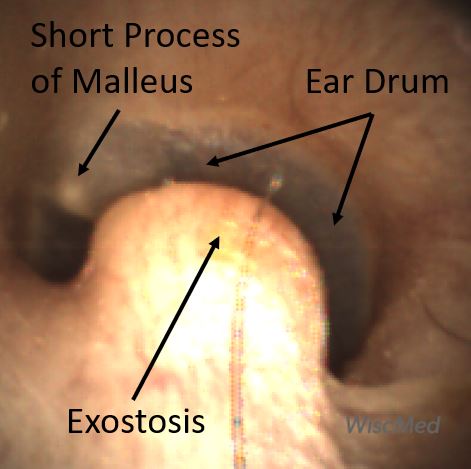
- Exostosis
-
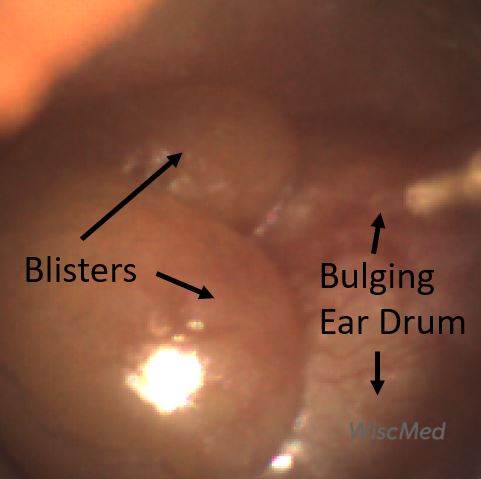
- Bullous Myringitis
WiscMed has created a visual guide to ear diagnosis that may be found here.
Here is the complete video exam. Note the power of the Wispr to navigate past ear wax.

Still not convinced? Click Here for a Free Trial