Otitis Media with Effusion
A 3-year-old presents to the pediatric emergency department (ED) with a chief complaint of wheezing. She has had several days of nasal congestion and was seen in an urgent care the prior evening where she was diagnosed with acute otitis media (AOM) and started on amoxicillin. The evening of presentation she was having shortness of breath. Her parents brought her in for evaluation. On physical exam, she is afebrile with a RR 40, HR 156, and Pox 96% on room air. She has mild course breath sounds bilaterally but no wheezing or increased work of breathing.
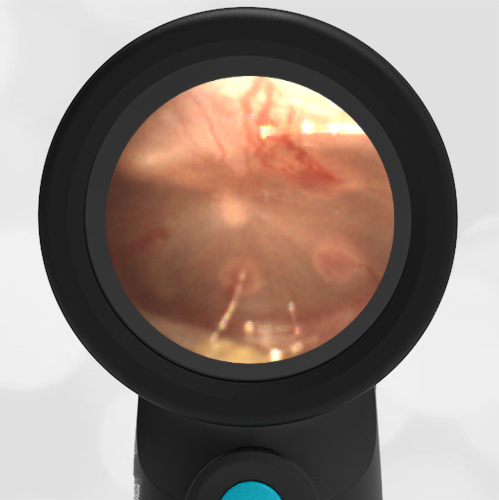
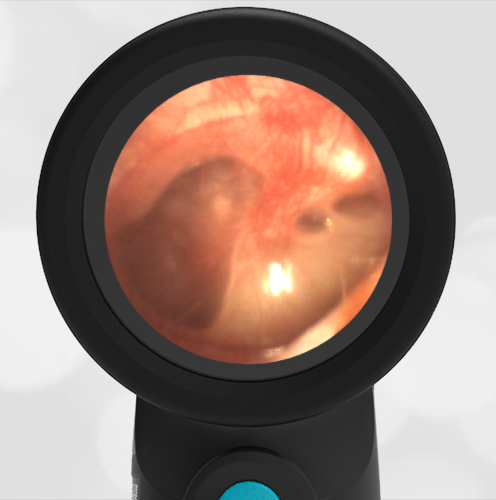
Her Wispr exam is notable for this image.
True or False:
This child should continue her amoxicillin.
False. The child has otitis media with effusion (OME). Antibiotics are not indicated.
Discussion:
This child’s Wispr exam demonstrates a mildly retracted tympanic membrane (TM) as evidenced by the slightly prominent malleus and a smaller, displaced light reflex. An additional finding is the presence of a yellowish/amber effusion inferiorly, thus her diagnosis is consistent with otitis media with effusion (OME). OME may be present in the setting of a resolving acute otitis media (AOM) or eustachian tube obstruction (i.e. an upper respiratory infection in a child) without infection, therefore antibiotics are not warranted.
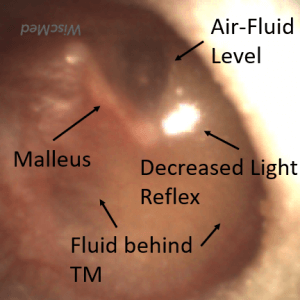
Various changes including air-fluid levels behind the TM, amber or gray color, displacement of the light reflex, mild to severe retraction, and accentuated landmarks are hallmarks of OME. This is in contrast to AOM in which mild to moderate bulging is the most sensitive indicator of bacterial infection. It is worth repeating that visualization of the tympanic membrane is critical to differentiate between AOM and OME and prevent the unnecessary prescription of antibiotics. The child in this case was discharged home with supportive measures for her respiratory illness and the recommendation to discontinue antibiotics. Most cases of OME resolve spontaneously in two to four weeks. Follow-up with a family physician is recommended if parents have ongoing concerns.